Abstract
Background: Nimesulide shows preferential inhibition for the cyclooxygenase-2 (COX-2) enzyme, which blocks the formation of prostaglandins critical in pain and inflammatory pathways. Few studies in the past have reported rare and unpredictable hepatic effects with nimesulide. The present study aimed to evaluate the efficacy and safety of nimesulide/paracetamol (100 mg + 325 mg) fixed-dose combination twice a day for 2 weeks in the management of acute pain in Indian population. Materials and methods: This was a multicenter study, performed on 500 patients, by 24 experienced physicians across India. The primary outcome assessed clinical safety at 2 weeks for mild/serious adverse effects (AEs), change in liver function tests (LFTs), serum bilirubin and alkaline phosphatase levels. The secondary outcomes assessed the clinical effectiveness in reduction of pain at rest and at movement. Results: Analysis of LFT at 2 weeks showed a slight increase (mean change) in the aspartate transaminase {-0.73 [95% confidence interval (CI) -1.54, 0.09; p = 0.081]}, alanine transaminase [-1.73 (95% CI -2.82, -0.64; p = 0.002)], serum bilirubin [-0.02 (95% CI -0.04, -0.001; p = 0.018)] and alkaline phosphatase levels [-1.92 (95% CI -5.84, 2; p = 0.336), not exceeding the normal range. Only one in 500 patients reported AEs. The numerical rating scale (NRS) scores for intensity of pain at rest and at movement at 2 weeks, ≤7 days and >7 days were 68.38%, 68.44% and 68.39%; and 65.43%, 64.60% and 66.02%, respectively. An improvement of 96.6% was observed in patient global assessment scale (GAS) and 97.2% in physician GAS. Conclusion: Nimesulide/paracetamol combination was safe, effective and well-tolerated in acute pain conditions and did not lead to clinically significant changes in liver parameters indicating hepatic safety.
Keywords: Nimesulide, paracetamol, acute pain, hepatic safety, COX-2 inhibitor
Pain is among the most frequent complaints encountered in clinical practice.1 Acute pain is a red flag for a disease or a threat to the body by a noxious insult and is expected to resolve within the normal anticipated healing period.2 Unrelieved or undertreated acute pain can lead to chronic pain.2 Nonsteroidal anti-inflammatory drugs (NSAIDs) are the cornerstone of acute pain management.2 They are a chemically diverse group of drugs that share similar therapeutic anti-inflammatory, analgesic and antipyretic properties, with the exception of the cyclooxygenase (COX)-2-selective agents.2 The most important property of NSAIDs is the reduction of the biosynthesis and accumulation of prostaglandins at the site of injury or inflammation by inhibition of the cyclooxygenases (COX-1 and the inducible COX-2).2 Their analgesic and anti-inflammatory properties make NSAIDs, the treatment of choice for relieving pain due to local inflammation.1 However, treatment with NSAIDs must be short-term and well-tolerated to overcome the painful syndrome at an acute stage leading to a quicker and easier recovery, owing to the tendency for spontaneous remission.1
Nimesulide is a unique, nonselective NSAID, which preferentially inhibits the COX-2 enzyme, that blocks the formation of prostaglandins critical in pain and inflammatory pathways.2 The relative specificity of nimesulide for COX-2 activity, attributes a close association to pain pathways as opposed to COX-1, which has major effects on gastric mucosa cell protection and platelet function.2 In India, nimesulide has been used for the treatment of acute pain due to trauma and acute musculoskeletal disorders such as tendinitis, sprains, strains, soft-tissue injury and myalgia, low back pain (LBP), pain due to dental, orthopedic and other minor surgeries in adults.2,3
Liver damage is a rare but well-recognized adverse event associated with the entire NSAID drug class.2 Studies have reported that about 15% patients taking NSAIDs experience at least transient serum aminotransferase elevations; however, a lower rate has been reported with nimesulide.2 Only less than 1% patients report greater than threefold elevation in aminotransferase level with nimesulide therapy and in majority of the cases, elevated serum aminotransferase levels are transient, mild and asymptomatic, and may resolve even when the drug is used in continuum.4
The onset of symptoms is usually 1 to 4 months after commencing therapy.5 Liver injury usually resolves 2 to 16 months after drug withdrawal.5 Recent pharmacoepidemiological studies concluded that the safety concerns with nimesulide are not higher compared with other NSAIDs, and the risk/benefit profile for hepatic side effects is comparable with other drugs in this class.2
Nimesulide is used in more than 50 countries, and is the most prescribed NSAID in Italy and Portugal, with Italy accounting for half the worldwide market.6 Some studies have reported rare and unpredictable hepatic injury with nimesulide therapy.2 However, in 2012, the European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) concluded that the benefits of systemic nimesulide-containing medicines outweigh their risks in the treatment of acute (short-term) pain, symptoms of painful osteoarthritis and primary dysmenorrhea when the dose of nimesulide was 100 mg twice a day and the duration of treatment was limited to a window of 15 consecutive days.2 The Drugs Controller General of India (DCGI) approved nimesulide in 1995 for pain and inflammatory conditions.7 In severe pain after extraction of impacted third molars or other dental procedure-associated pain, postoperative pain, the onset of therapeutic effect of nimesulide was faster (less than 15 minutes) it was stronger (according to patients’ opinion) than ibuprofen. In another study, nimesulide was found to be more effective in relieving pain in osteoarthritis of the hip and knees, with faster onset of action and fewer side effects than diclofenac and celecoxib.8 Nimesulide is readily available, and maximally inhibits the COX-2 enzyme at a high dose.
However, till date, to the best of our knowledge, there are no published studies using systematic evaluation methods to quantitatively assess the safety profile of nimesulide related to hepatotoxicity in peer reviewed journals especially in Indian population.
Thus, the present study was planned to evaluate the safety and efficacy of nimesulide/paracetamol fixed-dose combination in Indian adult patients with acute pain due to acute musculoskeletal disorders and trauma such as tendinitis, sprains, strains, soft-tissue injury and myalgia, LBP, pain due to dental, orthopedic and other minor surgeries.
MATERIALS AND METHODS
This SAFE (SUMO in Acute pain management: saFety and Efficacy) study was a prospective, open-label, observational, multicenter study conducted by 24 experienced physicians across India on 500 patients to evaluate the efficacy and safety of nimesulide/paracetamol (100 mg + 325 mg) fixed-dose combination. Independent Ethics Committee approval was taken and the study was conducted in accordance with the International Conference on Harmonization (ICH) for Good Clinical Practice (GCP) and the applicable Indian regulatory guidelines. An informed consent was obtained from all the patients prior to each patient enrollment after proper explanation of the study details, risks and benefits associated in their own regional language.
Data pertaining to all the required fields in order to fulfill the primary and secondary endpoints of the study were captured in a paper case record form (CRF). Data from the paper CRF were then transferred to an electronic-CRF (e-CRF) portal. This e-CRF portal is 21 CFR Part 11 & Health Insurance Portability and Accountability Act (HIPAA) compliant. Data entry, data query generation and resolution, source document verification and database lock were performed as per standard GCP guidelines.
Patients’ demographics were recorded in the form of age, weight, heart rate, blood pressure and comorbidities. Indian patients aged 18 years or older with acute painful conditions such as tendinitis, myalgia, LBP, sprains, pulled muscle, soft-tissue injury and dental pain, dental procedure/surgery were enrolled in the study. Pregnant or lactating females, patients having hepatic, renal or cardiac diseases, and those with history of hypersensitivity to the drug were strictly excluded from the study. Eligible patients were prescribed a daily dose of nimesulide/paracetamol (100 mg + 325 mg) twice a day after meals for a duration of 3-14 days as per the physician’s discretion.
The primary outcomes of the study included safety endpoints that were assessed, based on the altered liver enzyme levels; aspartate transaminase (AST)/serum glutamic-oxaloacetic transaminase (SGOT), alanine transaminase (ALT)/serum glutamic-pyruvic transaminase (SGPT), serum bilirubin and alkaline phosphatase levels. The proportion of subjects with adverse effects (AEs) and severe adverse effects (SAEs) and the intensity of AEs and SAEs at baseline and at the end of treatment were also evaluated. The secondary outcomes included clinical efficacy endpoints assessed and observed, based on the numerical rating scale (NRS) and physician/patient global assessment scale (GAS) at baseline and at the end of treatment. The NRS scores were calculated on a 10-point rating scale, with scores ranging from 0 to 10, where 0: no pain; 1-3: mild pain; 4-6: moderate pain and 7-10: severe pain. The GAS scores were rated according to a 5-point rating scale where 1: complete relief of symptoms; 2: marked improvement of symptoms; 3: moderate improvement of symptoms; 4: slight improvement of symptoms and 5: no change in symptoms.
All qualitative parameters were summarized by frequency and percentage and quantitative variables by descriptive statistics such as mean and standard deviation (SD). The within group change p value was derived by paired t-test, and the between group change p value was derived by independent t-test. The mean changes within the groups and between the groups (p value) were compared by paired t-test and independent t-test, respectively. The changes across indications were compared by analysis of variance (ANOVA). A p value <0.05 was considered as statistical significance. The data were analyzed by statistical software R version 4.1.0 (R Core Team, 2021, Vienna, Austria).
RESULTS
A total of 513 patients were enrolled in the study of which 500 patients completed the study. The demographic analysis of 466 records showed the mean age of 40 years. The mean weight was 65.82 kg (n = 432). The baseline characteristics of the patients enrolled are shown in Table 1. The diagnosis was based as per the discretion of the treating clinician with major reported complaints such as myalgia, LBP, dental pain and other indications such as pulled muscle, soft-tissue injuries, sprains, tendinitis and traumatic pain. Few patients had comorbidities including hypertension, type 2 diabetes mellitus, gastric illness, liver disease and other illnesses.
|
Table 1. Baseline Characteristics of Study Participants
|
|
Characteristic
Age (years), mean
Weight (kg), mean
|
40.1
65.8
|
|
Gender (n = 500)
Male
Female
|
No (%)
202 (40.4)
298 (59.6)
|
|
Comorbidities (n = 84)
Hypertension
Type 2 diabetes mellitus (T2DM)
Gastric illness
Liver disease
Others
|
No (%)
37 (44.0)
33 (39.3)
3 (3.6)
2 (2.4)
9 (10.7)
|
|
Underlying painful condition (n = 463)
Myalgia
Low back pain
Dental pain
Others (pulled muscle, soft-tissue injuries, sprains, tendinitis and traumatic pain)
|
No (%)
149 (32.2)
108 (23.3)
80 (17.3)
126 (27.2)
|
Of all the patients, only 1 patient (history of diabetes, hypertension and gastric illness) reported periorbital swelling and pedal edema (1 in 500). Apart from this patient, none of the study participants reported any mild/SAEs at the end of treatment with nimesulide/paracetamol combination. The liver function tests (LFTs) were performed on all participants and the values before and after the treatment did not show any significant change in AST/SGOT, ALT/SGPT, serum bilirubin and alkaline phosphatase levels during the treatment period. The mean and SD of LFT parameters between baseline and endline by paired t-test and mean change with 95% confidence interval (CI) were also reported. Change was measured by baseline to endline, therefore negative change means increase. Analysis of LFTs during the treatment duration of ≤7 days vs. >7 days showed a slight increase in the AST/SGOT [-0.27 (95% CI -1.67 to 1.12) vs. -1.01 (95% CI -2.02 to -0.01); p = 0.398], ALT/SGPT [-0.81 (95% CI -2.18 to 0.56) vs. -2.32 (95% CI -3.88 to -0.76); p = 0.151], serum bilirubin [0 (95% CI -0.03 to 0.03) vs. -0.03 (95% CI -0.05 to -0.01); p = 0.063], and alkaline phosphatase levels [-2.01 (95% CI -9.18 to 5.16) vs. -1.86 (95% CI -6.41 to 2.69); p = 0.973], but did not exceed the normal range of the tested parameters (Table 2; Fig. 1 a-d).
|
Table 2. Analysis of LFT Parameters (During Treatment Duration)
|
|
Parameter
|
Group
|
Pre: Mean (SD)
|
Post: Mean (SD)
|
Within group change (95% CI)
|
Between group change (95% CI)
|
|
AST/SGOT
|
≤7 d
>7 d
|
28.45 (12.39)
28.34 (10.9)
|
28.73 (14.84)
29.35 (12.59)
|
-0.27 (-1.67 to 1.12)
-1.01 (-2.02 to -0.01)
|
0.74 (-0.98 to 2.45)
P = 0.398
|
|
ALT/SGPT
|
≤7 d
>7 d
|
30.2 (16.76)
28.92 (14)
|
31.01(18.93)
31.25 (15.72)
|
-0.81 (-2.18 to 0.56)
-2.32 (-3.88 to -0.76)*
|
1.51 (-0.56 to 3.58)
P = 0.151
|
|
Serum bilirubin
|
≤7 d
>7 d
|
0.57 (0.28)
0.62 (0.31)
|
0.57 (0.27)
0.65 (0.29)
|
0 (-0.03 to 0.03)
-0.03 (-0.05 to -0.01)*
|
0.03 (0 to 0.06)
P = 0.063
|
|
Alkaline phosphatase
|
≤7 d
>7 d
|
121.18 (66.92)
128.06 (75.38)
|
123.19 (80.55)
129.92 (71.97)
|
-2.01 (-9.18 to 5.16)
-1.86 (-6.41 to 2.69)
|
0.15 (-8.62 to 8.32)
P = 0.973
|
*Indicates statistical significance (p value < 0.05).
LFT = Liver function test; SD = Standard deviation; CI = Confidence interval; AST = Aspartate transaminase; SGOT = Serum glutamic-oxaloacetic transaminase; ALT = Alanine transaminase; SGPT = Serum glutamic-pyruvic transaminase.
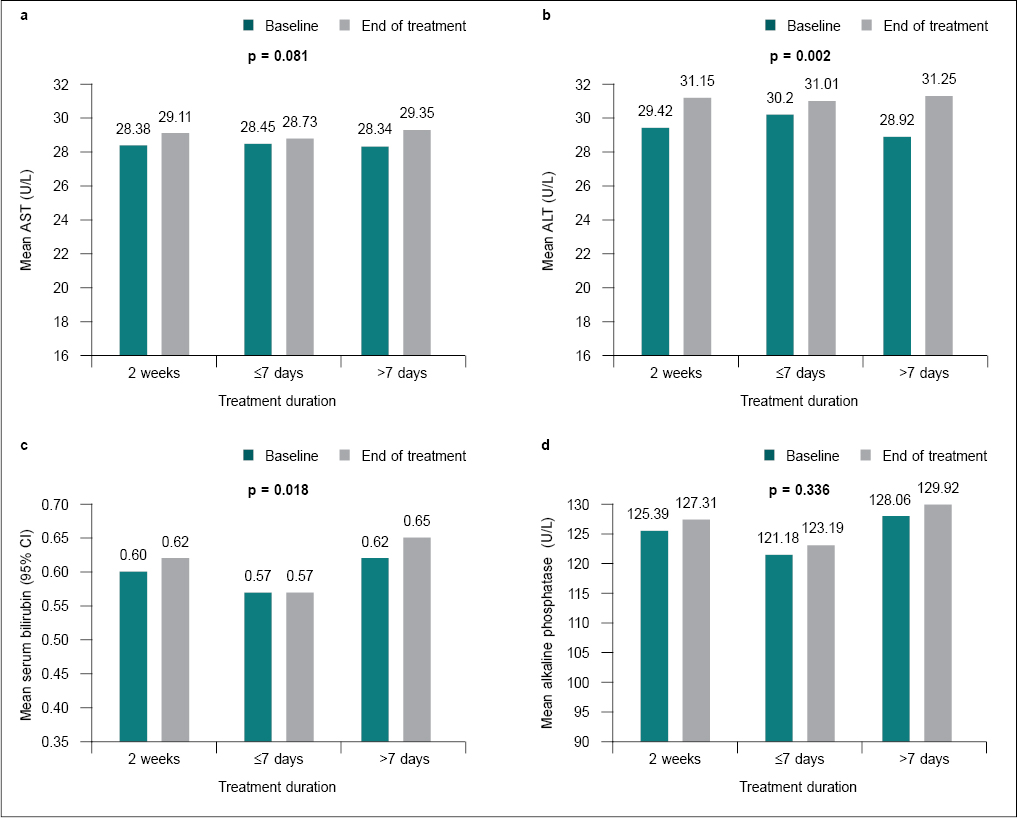
Figure 1. Mean comparison with 95% CI between baseline and end of treatmentfor all LFT parameters. (a) Mean comparison for treatment duration of AST, (b) Mean comparison for treatment duration of ALT, (c) Mean comparison for treatment duration of serum bilirubin and (d) Mean comparison for treatment duration of alkaline phosphatase.
Analysis of LFTs at the end of treatment showed no significant increase (mean change) in the AST/SGOT [-0.73 (95% CI -1.54 to 0.09); p = 0.081], ALT/SGPT [-1.73 (95% CI -2.82 to -0.64); p = 0.002], serum bilirubin [-0.02 (95% CI -0.04 to -0.001); p = 0.018] and alkaline phosphatase levels [-1.92 (95% CI -5.84 to 2); p = 0.336]. Thus, all the LFTs were reported to be in the normal range of the tested parameters (Table 3; Fig. 1 a-d).
|
Table 3. Analysis of LFT Parameters at the End of Treatment
|
|
Variables
|
Period
|
N
|
Mean (SD)
|
Mean change (95% CI)
|
P value
|
|
AST/SGOT
|
Baseline
Endline
|
500
500
|
28.38 (11.49)
29.11 (13.5)
|
-0.73 (-1.54 to 0.09)
|
0.081
|
|
ALT/SGPT
|
Baseline
Endline
|
500
500
|
29.42 (15.13)
31.15 (17.02)
|
-1.73 (-2.82 to -0.64)
|
0.002
|
|
Serum bilirubin
|
Baseline
Endline
|
500
500
|
0.6 (0.3)
0.62 (0.28)
|
-0.02 (-0.04 to -0.001)
|
0.018
|
|
Alkaline phosphatase
|
Baseline
Endline
|
500
500
|
125.39 (72.23)
127.31 (75.41)
|
-1.92 (-5.84 to 2)
|
0.336
|
The secondary outcomes included analysis of NRS scores for the intensity of pain at rest and movement during treatment and at the end of the study. Analysis of NRS at rest during the treatment duration of ≤7 days showed that the mean change within the groups was 3.35 (95% CI 3.09 to 3.6); p < 0.05 and 3.29 (95% CI 3.06 to 3.53); p < 0.05 for treatment duration of >7 days (Table 4). Analysis of NRS at movement during the treatment duration of ≤7 days showed that the mean change within the groups was 3.65 (95% CI 3.39 to 3.91); p < 0.05 and for treatment duration of >7 days, it was 3.75 (95% CI 3.5 to 4); p < 0.05 (Table 4). The study showed that nimesulide/paracetamol combination demonstrated significant reduction in the pain intensity at rest [4.88 (1.43) vs. 1.54 (1.3); p < 0.05; (Fig. 2; Table 4)] in the first 7 days and [4.81 (1.71) vs. 1.52 (1.37); p < 0.05; (Fig. 2; Table 4)] for treatment duration of >7 days. A significant reduction in the pain intensity was also observed at movement during the initial 7 days [5.65 (1.54) vs. 2 (1.23); p < 0.05; (Fig. 3; Table 4)] and [5.68 (1.76) vs. 1.93 (1.35); p < 0.05; (Fig. 3; Table 4)] for treatment duration of >7 days.
|
Table 4. Analysis of NRS Scores for Intensity of Pain at Rest and Movement During Treatment
|
|
Variable
|
Group
|
Pre:
Mean (SD)
|
Post:
Mean (SD)
|
Within group change (95%CI)
|
Between group change (95%CI)
|
% Reduction
|
|
NRS at rest
|
≤7 d
>7 d
|
4.88 (1.43)
4.81 (1.71)
|
1.54 (1.3)
1.52 (1.37)
|
3.35 (3.09 to 3.6)*
3.29 (3.06 to 3.53)*
|
0.05 (-0.29 to 0.39)
P = 0.769
|
68.44
68.39
|
|
NRS at movement
|
≤7 d
>7 d
|
5.65 (1.54)
5.68 (1.76)
|
2 (1.23)
1.93 (1.35)
|
3.65 (3.39 to 3.91)*
3.75 (3.5 to 4)*
|
0.1 (-0.46 to 0.25)
p = 0.574
|
64.6
66.02
|
*P < 0.05
NRS = Numerical rating scale.
NRS scores at baseline vs. at the end of treatment showed significant reduction in the pain intensity at rest (4.84 vs. 1.53; p < 0.001; Fig. 2; Table 5) and at movement (5.67 vs. 1.96; p < 0.001; Fig 3; Table 5), respectively.
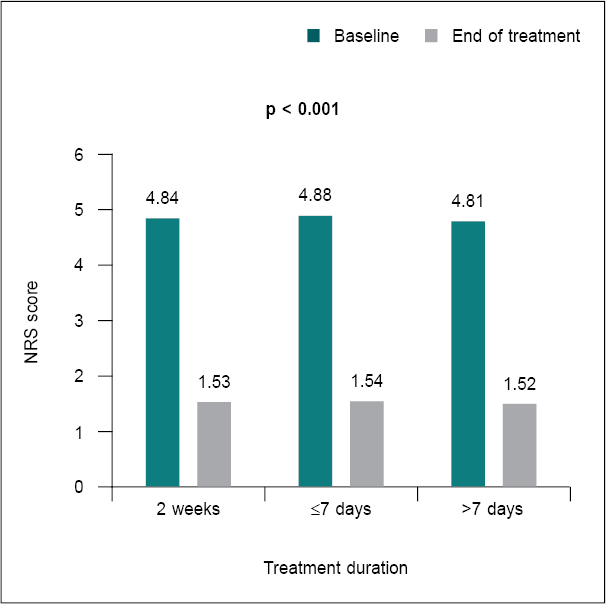
Figure 2. Mean comparison of NRS scores during treatment duration for pain intensity at rest.
|
Table 5. Analysis of NRS Scores for Intensity of Pain at Rest and Movement at the End of Treatment
|
|
Variable
|
Period
|
N
|
Mean (SD)
|
Mean reduction (95% CI)
|
P value
|
% Reduction
|
|
NRS at rest
|
Baseline
Endline
|
500
500
|
4.84 (1.61)
1.53 (1.34)
|
3.31 (3.14 to 3.49)
|
<0.001
|
68.38
|
|
NRS at movement
|
Baseline
Endline
|
500
500
|
5.67 (1.67)
1.96 (1.3)
|
3.71 (3.53 to 3.89)
|
<0.001
|
65.43
|
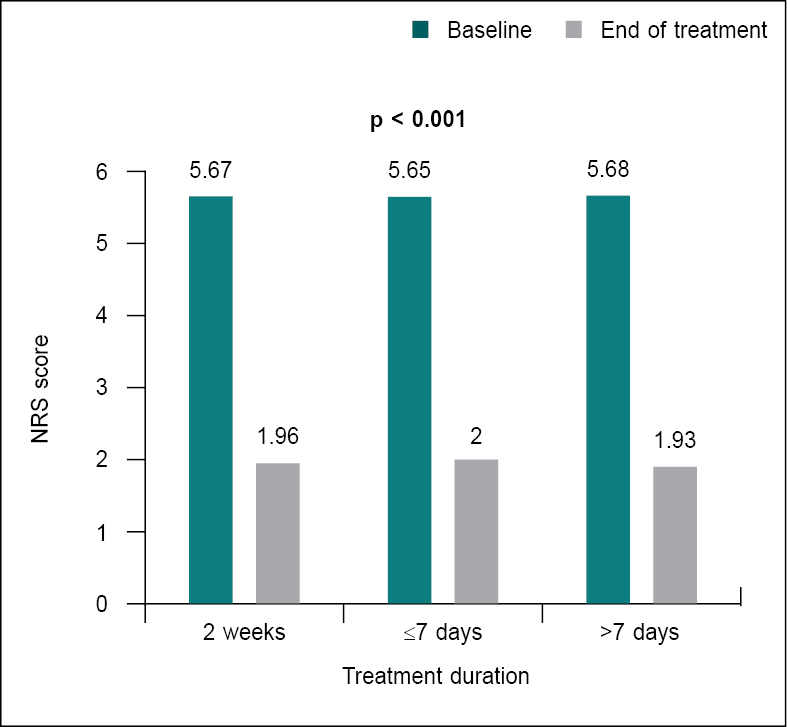
Figure 3. Mean comparison of NRS score during treatment duration for pain intensity at movement.
The reduction in NRS scores for the intensity of pain at rest, ≤7 days and >7 days were reported to be 68.44% and 68.39%; p < 0.05 (Table 4). At the end of treatment, the reduction in NRS scores for intensity of pain at rest was observed to be be 68.38%; p < 0.001, respectively (Table 5).
The reduction in NRS scores for the intensity of pain at movement, ≤7 days and >7 days were reported to be 64.60% and 66.02%; p < 0.05 (Table 4). At the end of treatment, the reduction in NRS scores for intensity of pain at movement was observed to be 65.43%; p < 0.001, respectively (Table 5).
The patient GAS within 7 days vs. >7 days was 1.85 vs. 1.94; p = 0.19 and the physician GAS was 1.80 vs. 1.97; p = 0.022, respectively (Table 6). The patient and physician GAS at ≤7 days, >7 days and at the end of the treatment showed marked improvement in symptoms in 96.6% patient GAS and 97.2% physician GAS (Table 7).
|
Table 6. Comparison of GAS Patient and Physician in GAS
|
|
Parameter
|
Group
|
N
|
Mean
|
SD
|
P value
|
|
Patient global assessment
|
≤7 d
>7 d
|
194
306
|
1.8505
1.9477
|
0.7841
0.8399
|
0.19
|
|
Physician global assessment
|
≤7 d
>7 d
|
194
306
|
1.8041
1.9706
|
0.7637
0.8273
|
0.022
|
GAS = Global assessment scale.
|
Table 7. Patient and Physician GAS for Improvement in Symptoms
|
|
Parameters
|
Patient GAS (N = 500)
|
|
|
Physician GAS (N = 500)
|
|
Count
|
%
|
Count
|
%
|
|
1 = Complete relief of symptoms
|
175
|
35
|
172
|
34.4
|
|
2 = Marked improvement of symptoms
|
212
|
42.4
|
218
|
43.6
|
|
3 = Moderate improvement of symptoms
|
96
|
19.2
|
96
|
19.2
|
|
4 = Slight improvement of symptoms
|
17
|
3.4
|
13
|
2.6
|
|
5 = No change in symptoms
|
-
|
-
|
1
|
0.2
|
N = Number of study participants.
DISCUSSION
Nimesulide has been in clinical use for more than three decades and is still sustained owing to its effectiveness in controlling pain and inflammation as well as its favorable safety profile with regard to a reduced propensity to cause adverse gastrointestinal effects.2,9 The gastrointestinal absorption of nimesulide is rapid and complete, and it gets rapidly distributed in the synovial fluid, where it persists for a longer duration than blood, thus explaining its effectiveness in pain control.10 From the perspective of safety, the preferential activity of nimesulide on COX-2 attributes to a lower risk of upper gastrointestinal bleeding.10 In patients with moderate renal impairment, the pharmacokinetic profiles of nimesulide are not altered.2
In the present multicenter, open-label study, nimesulide/paracetamol combination was well-tolerated and only 1 patient experienced AEs with the drug combination. Except this patient, none experienced any mild/serious AEs and continued the treatment as directed. The no/low incidence of AEs of nimesulide, may be attributed to the preferential COX-2 inhibition, thus a lower potential for gastrointestinal side effects.2,4
In the present study, the primary outcomes involved assessment of patients for changes in LFTs including ALT, AST, serum bilirubin and alkaline phosphatase levels when given nimesulide/paracetamol fixed-dose combination. Though a very mild increase in the liver aminotransferase levels were reported in the study patients, they were within the normal range of the tested parameters. Comparable inferences can be drawn from the results of a post-marketing surveillance study of patients prescribed nimesulide and assessed for LFTs which reported that ALT, AST and serum bilirubin values post-nimesulide treatment remained unaltered.11
In this study, the effectiveness of nimesulide/paracetamol combination was assessed and observed using NRS score over a short period of 3-14 days of treatment in relieving pain at rest and at movement, in patients suffering from painful conditions. A significant reduction in the degree of pain was observed based on the evaluation of the NRS scores, for the intensity of pain at rest on the 7th day of treatment, which was 1.54 points and at movement, reported as 2 points. These observations indicate the anti-inflammatory and analgesic effects of the studied combination by effectively restoring the functions in patients with painful conditions. The study findings were in accordance with a similar study conducted by Shikhkerimov et al on 54 patients to assess the efficacy and safety of nimesulide 200 mg/day in the treatment of acute LBP.12 The analysis took into account assessment of the pain intensity at rest and at movement. Treatment with nimesulide resulted in pain relief and increased mobility in the lumbar spine on the 5th day of treatment indicating effectiveness to restore the previous functional status of patients with LBP.12
Marked improvement was observed in symptoms at the end of the treatment based on the GAS scores for patients reported as 96.6% and GAS scores of physicians was reported to be 97.2%, respectively. These results were comparable to a study conducted by Khan et al on 125 Indian patients with soft-tissue injuries and had been prescribed nimesulide for a period of 7 days.13 The study demonstrated that the GAS was rated as “good” by both physicians (88.7%) as well as patients (83.9%).13 The overall treatment compliance was very good leading to the conclusion that nimesulide is well-accepted by the patients and enhances the treatment adherence. 13
All the participants in the present study completed the trial and only one reported AEs. Our study showed that the incidence of adverse events was low with the fixed-dose combination of nimesulide/paracetamol. The laboratory investigations of LFTs including SGOT, SGPT, serum bilirubin and alkaline phosphatase levels were done as suggested by the physicians. All patients underwent these tests and none of the patients reported any significant change in the tested parameters. These observations indicate that nimesulide/paracetamol combination demonstrates no potential role with respect to clinically significant increase in LFTs when used for a period of 3-14 days. Majority of the patients showed significant reduction in the pain intensity at rest and at movement, and an improvement in symptoms during the treatment period assessed using the NRS scores and the patient and physician GAS scores. Overall, our study showed that nimesulide/paracetamol combination was observed to be a safe and effective regimen with good tolerability profile in patients with acute pain conditions.
CONCLUSION
The SAFE study showed that the incidence of altered LFTs with nimesulide/paracetamol combination treatment was rare and at par with other conventional NSAIDs. Nimesulide/paracetamol combination given for acute painful conditions for a duration of 3 to 14 days, sporadically showed no clinically significant change in the liver enzymes elucidating the hepatic safety of this combination. Based on the LFT parameters, NRS and GAS scores, the nimesulide/paracetamol fixed-dose combination was safe and clinically effective for use in acute pain conditions.
Acknowledgment
The study was conducted by Alkem Laboratories Ltd.
Insignia Communications Pvt. Ltd. managed the overall execution of the study and also carried out the analysis and drafted the manuscript.
Dr Priti Sarma, Medical Affairs Department, Alkem Laboratories Ltd. contributed in the revision of the final version of the manuscript.
Funding
This study was funded by Alkem Laboratories Ltd.
Conflict of Interest
None
Informed Consent Statement
The work represented has been carried out in an ethical way. Informed consent was obtained from all the Investigators and study subjects who took part in the study.
REFERENCES
- Famaey JP, Vandekerckhove K, Geczy J, Bruhwyler J. A large, open-label trial of nimesulide in patients with osteoarticular conditions treated in a general practice setting. Curr Ther Res. 1998;59(7):467-82.
- Kress HG, Baltov A, Basinski A, Berghea F, Castellsague J, Codreanu C, et al. Acute pain: a multifaceted challenge - the role of nimesulide. Curr Med Res Opin. 2016;32(1):23-36.
- Arulrhaj S, Tiwaskar M, Sabharwal M, Saikia R, Majid S, Rathod R, et al. Effectiveness of nimesulide in acute fever management in adults: retrospective electronic medical records database study outcome in outpatient department. J Assoc Physicians India. 2021;69(7):11-2.
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet] [Updated Mar 1, 2016]. Available from: https://pubmed.ncbi.nlm.nih.gov/3163176/. Accessed Mar 24, 2022.
- Aithal GP, Day CP. Nonsteroidal anti-inflammatory drug-induced hepatotoxicity. Clin Liver Dis. 2007;11(3):563-75.
- Traversa G, Bianchi C, Da Cas R, Abraha I, Menniti-Ippolito F, Venegoni M. Cohort study of hepatotoxicity associated with nimesulide and other non-steroidal anti-inflammatory drugs. BMJ. 2003;327(7405):18-22.
- Central Drugs Standard Control Organisation. Directorate General of Health Services Ministry of Health & Family Welfare, Government of India. Available at: https://cdscoonline.gov.in/CDSCO/Drugs. Accessed July 01, 2022.
- Dalewski B, Kaminska A, Szydlowski M, Kozak M, Sobolewska E. Comparison of early effectiveness of three different intervention methods in patients with chronic orofacial pain: a randomized, controlled clinical trial. Pain Res Manag. 2019;2019:7954291.
- Kwon J, Kim S, Yoo H, Lee E. Nimesulide-induced hepatotoxicity: a systematic review and meta-analysis. PLoS One. 2019;14(1):e0209264.
- Mattia C, Ciarcia S, Muhindo A, Coluzzi F. Nimesulide 25 annidopo [Nimesulide: 25 years later]. Minerva Med. 2010;101(4):285-93.
- Chandanwale A, Naikwadi A, Jain S, Airan C, Dhusia H, Verma S, et al. Post marketing surveillance study of nimesulide in Indian population. Indian Medical Gazette. 2003;CXXXVII:112-22.
- Shikhkerimov RK. The use of nimesulide in the treatment of acute low back pain. Zh Nevrol Psikhiatr Im S S Korsakova. 2016;116(5):28-32.
- Khan MA, Rao M, Reddy MM, Tamloorker D, Gumdal V, Latha MS, et al. A phase III trial evaluating the efficacy and tolerability of nimesulide 1% spray in patients with soft-tissue injuries. Int J Crit Illn Inj Sci. 2013;3(1):18-24.